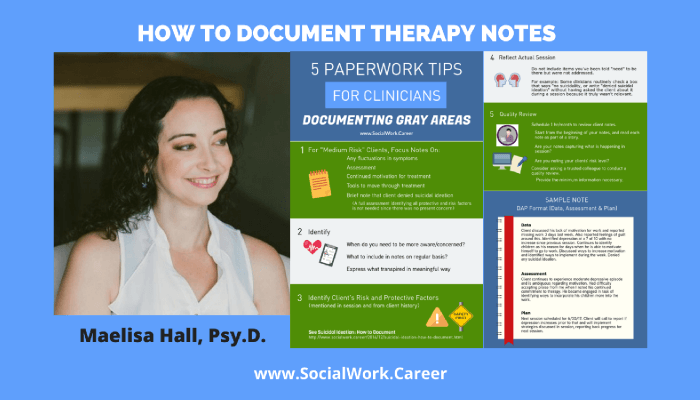
Not every therapy client is high-risk or worry-free—most fall somewhere in between. These “medium risk” situations include ongoing depression, self-harm behaviors without suicidal intent, impulsivity, and substance use. They require consistent assessment but don’t typically warrant hospitalization. The challenge? Knowing what to document and how often. This guide provides five practical tips from clinical documentation expert Maelisa Hall for managing therapy notes with medium risk clients. You’ll learn how to identify what’s truly relevant to document (without writing excessive notes), see a real DAP note example for a client with moderate depression, and discover why reviewing your documentation monthly can transform your practice. Whether you’re a new clinician or experienced therapist, these strategies help you create meaningful, legally sound therapy notes without burning out on paperwork
Suicidal Ideation: How to Document
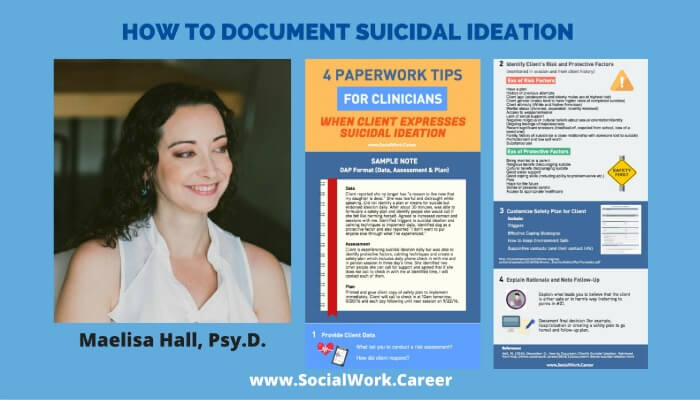
When a client expresses suicidal ideation, documentation becomes crucial but also anxiety-inducing for many clinicians. Learn the four key components of effective suicide risk assessment documentation: providing clear client data with exact quotes, identifying risk and protective factors, creating safety plans (not contracts), and explaining your clinical rationale. This guide includes a sample progress note using the DAP format and best practices for follow-up documentation. Whether you’re a new clinician or experienced practitioner, these principles will help you create ethically sound documentation that protects both you and your clients while improving clinical practice.
Social Work Internship: 12th Week

The other day at my placement was particularly difficult for me. One of my clients, let’s call her S, came in after having cut herself a few days earlier and as I questioned her, I learned that she had some suicidal ideation. In layman’s terms, this means that she expressed some wishes or fantasies about […]
